Trusted By
9,000+ Patients Globally
End-stage congestive heart failure in elderly patients is the final phase (Stage D) of heart failure, where the heart can no longer pump enough blood despite maximum medical therapy, and symptoms stay present even at rest. It usually brings severe breathlessness, fatigue, swelling, and declining organ function, and treatment decisions shift toward LVAD, transplant, or palliative care.
Dr. Vishal Khullar, an experienced Cardiac Surgeon in Mumbai, India, trained at Mayo Clinic and Cleveland Clinic, and currently the Director of the heart and lung transplant program at Fortis Mulund, has evaluated hundreds of elderly patients progressing into end-stage heart failure. This blog explains what end-stage CHF looks like in elderly patients, why it is often missed, and what realistic treatment options are available.
End-stage CHF means the heart muscle has weakened to the point where it can’t keep the rest of the body going, even with the best medications. It hasn’t stopped working, it just can’t keep up with demand. Blood backs up, fluid moves into the lungs and legs, and organs like the kidneys and liver begin to struggle because blood flow to them drops.
In elderly patients, this stage usually builds slowly. Years of high blood pressure, diabetes, old heart attacks, or valve problems wear the heart down bit by bit. At some point, the medications that are used to keep things under control just stop being enough. The patient starts spending more time in the hospital than at home. Simple activities become exhausting. And the family starts asking bigger questions about what comes next.
Some elderly patients are still early enough in the disease that options like heart bypass surgery or valve repair can meaningfully turn things around. But once end-stage hits, the conversation shifts to something entirely different.
Book a consultation with Dr. Vishal Khullar to understand your loved one’s heart condition and the right treatment path.

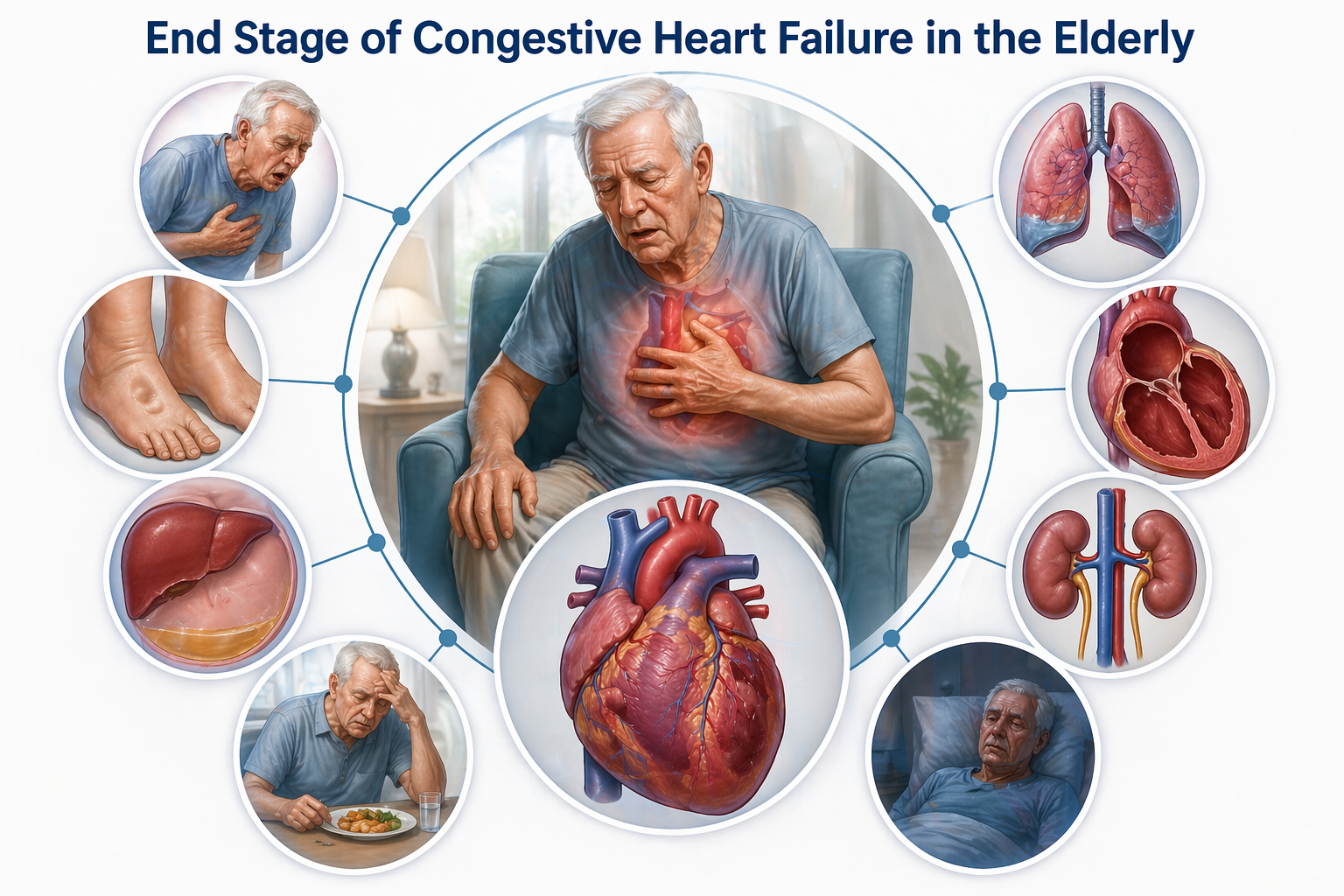
End-stage CHF doesn’t hide anymore. By this point, the symptoms are loud, they pile up, and they stop responding to the medicines that used to work.
The patient gets breathless just sitting up. Talking drains them. Lying flat feels impossible, so they start sleeping propped up on multiple pillows or in a chair. This isn’t a small thing; it’s often the clearest sign that the heart is overwhelmed.
Swelling in the legs, ankles, and abdomen that doesn’t respond to diuretics is a major red flag. The kidneys are retaining fluid because blood flow is poor. The veins are congested. And the body simply can’t clear the extra water.
This is one of the most telling signs. The same patient keeps coming back every few weeks for fluid overload, low output, or rhythm problems. Each admission leaves them a little weaker than before.
Called cardiac cachexia, this late sign is easy to miss because people assume the patient just isn’t eating well. What’s actually happening is the body is breaking down because chronic heart failure has started draining it of reserves.
Reduced blood flow to the brain causes new confusion or drowsiness. Atrial fibrillation or ventricular arrhythmias become more frequent. Ejection fraction on echocardiogram often sits below 20–25% despite full therapy. When three or more of these show up together, it’s no longer ordinary heart failure.
Here’s the real issue. In elderly patients, so many of these symptoms get dismissed as just getting older, and that’s what delays diagnosis.
Early recognition matters enormously. The window for meaningful intervention in elderly patients is narrower, and once it closes, it’s very hard to reopen.
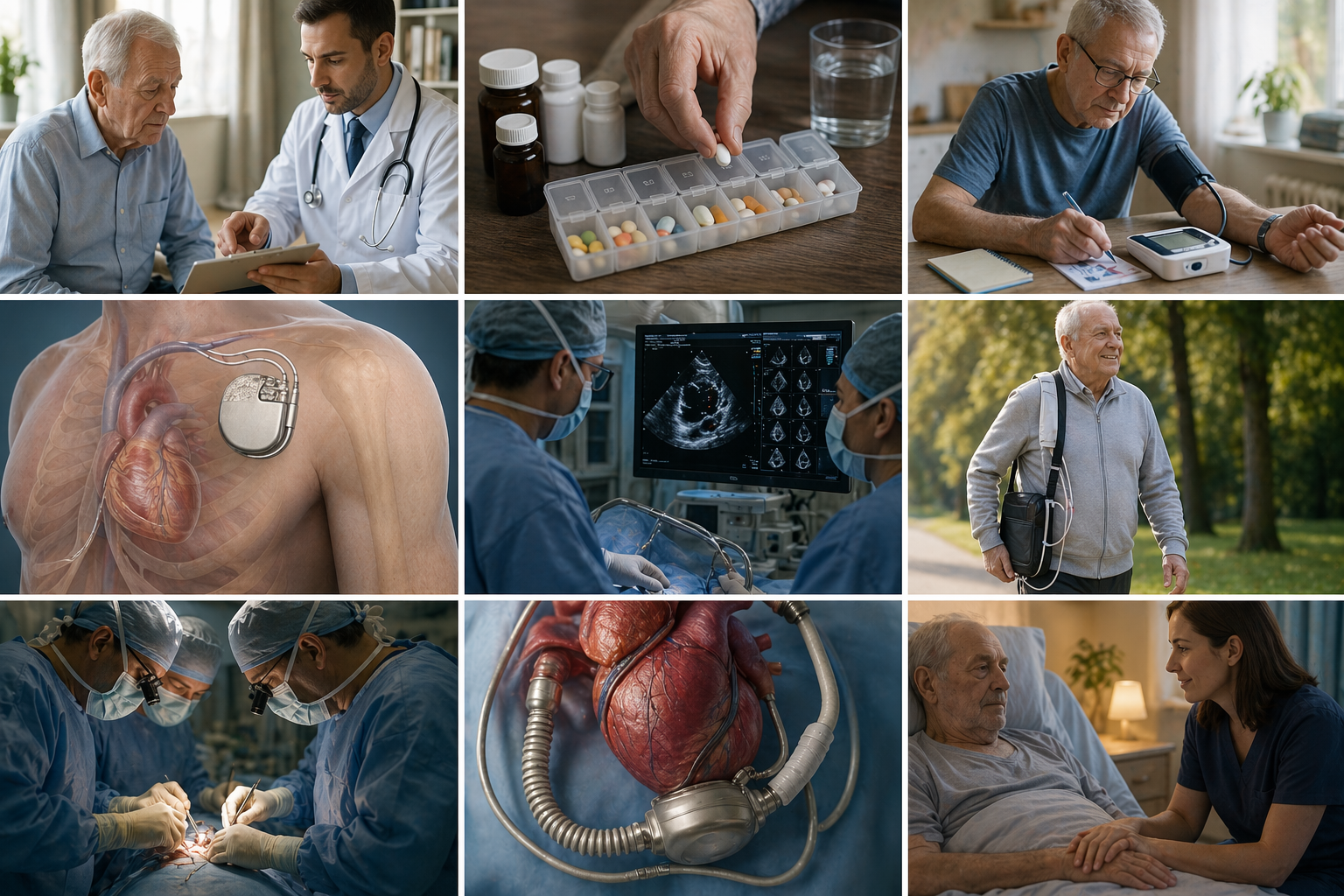
Treating end-stage CHF in elderly patients isn’t about one single procedure or medication. It’s about matching the right combination of care to the patient’s specific situation. There’s no one-size-fits-all plan.
Diuretics, beta-blockers, ACE inhibitors, ARNIs, and SGLT2 inhibitors are all titrated carefully. Elderly patients often can’t tolerate full doses because of kidney function or low blood pressure. Fluid and salt restriction become daily habits. Regular weight monitoring at home helps catch fluid retention before it becomes another hospital admission.
ICDs prevent sudden cardiac death from dangerous rhythms. CRT helps when the heart’s electrical system is out of sync. In carefully selected elderly patients, these devices genuinely extend life and improve symptoms in ways medications alone can’t.
For elderly patients with reversible causes, bypass or valve surgery can still be an option if the overall health supports it. When medications aren’t holding the line, an LVAD – Left Ventricular Assist Device becomes worth considering as destination therapy. It’s a mechanical pump that takes over the work the failing heart can no longer do. Many elderly patients on LVAD live well for years with a meaningful quality of life.
When aggressive treatment isn’t the right answer anymore, focus shifts to comfort, symptom control, and dignity. Palliative care isn’t giving up. It’s a different kind of active care, and it runs alongside cardiac treatment, not instead of it. For many elderly patients and their families, this becomes the most humane and meaningful path forward.
Here’s where expert judgment makes a real difference. Too aggressive too early, and an elderly patient is put through surgery they might not have needed. Too cautious, too long, and the opportunity for meaningful intervention passes. Neither extreme serves the patient.
Dr. Khullar regularly sees elderly patients referred late, when the heart and other organs have already been strained beyond reversible limits. Some still recover well with the right surgical or device-based plan. Others have lost too much organ reserve, and the conversation honestly shifts to palliative care at that point.
Something easily missed before things progress this far is heart valve diseases that can cause right-sided heart failure, which in elderly patients can accelerate decline rapidly if not picked up in time. An early cardiac evaluation by an experienced surgeon often separates good outcomes from missed windows.
Any advanced stage of heart failure carries real risks, and end-stage CHF in elderly patients is no different. Sudden cardiac death from arrhythmias is a genuine concern. Kidney and liver function tend to decline steadily. Infections, especially pneumonia, become harder to recover from. Repeated hospital stays wear down both the patient and the family.
None of this means treatment isn’t worth pursuing. It means decisions need to be made realistically, with eyes open, and with a cardiac team that understands when to push forward with intervention and when comfort becomes the priority. Getting this balance right is where real expertise matters most.
End-stage congestive heart failure in elderly patients is hard, but it isn’t without options. The problem is that signs get dismissed as normal aging, so the window for meaningful treatment often closes before anyone realizes it was open. Catching it early, recognizing what’s actually happening, and getting evaluated by an experienced cardiac surgeon makes a tremendous difference in what’s possible.
The question isn’t always whether your elderly loved one needs a transplant or an LVAD. It’s whether they’re being evaluated by someone who’s seen hundreds of these cases and knows what the realistic options actually are. Dr. Vishal Khullar’s experience with advanced heart failure in elderly patients means you get an honest, experienced opinion on where things stand and what comes next.




