Trusted By
9,000+ Patients Globally
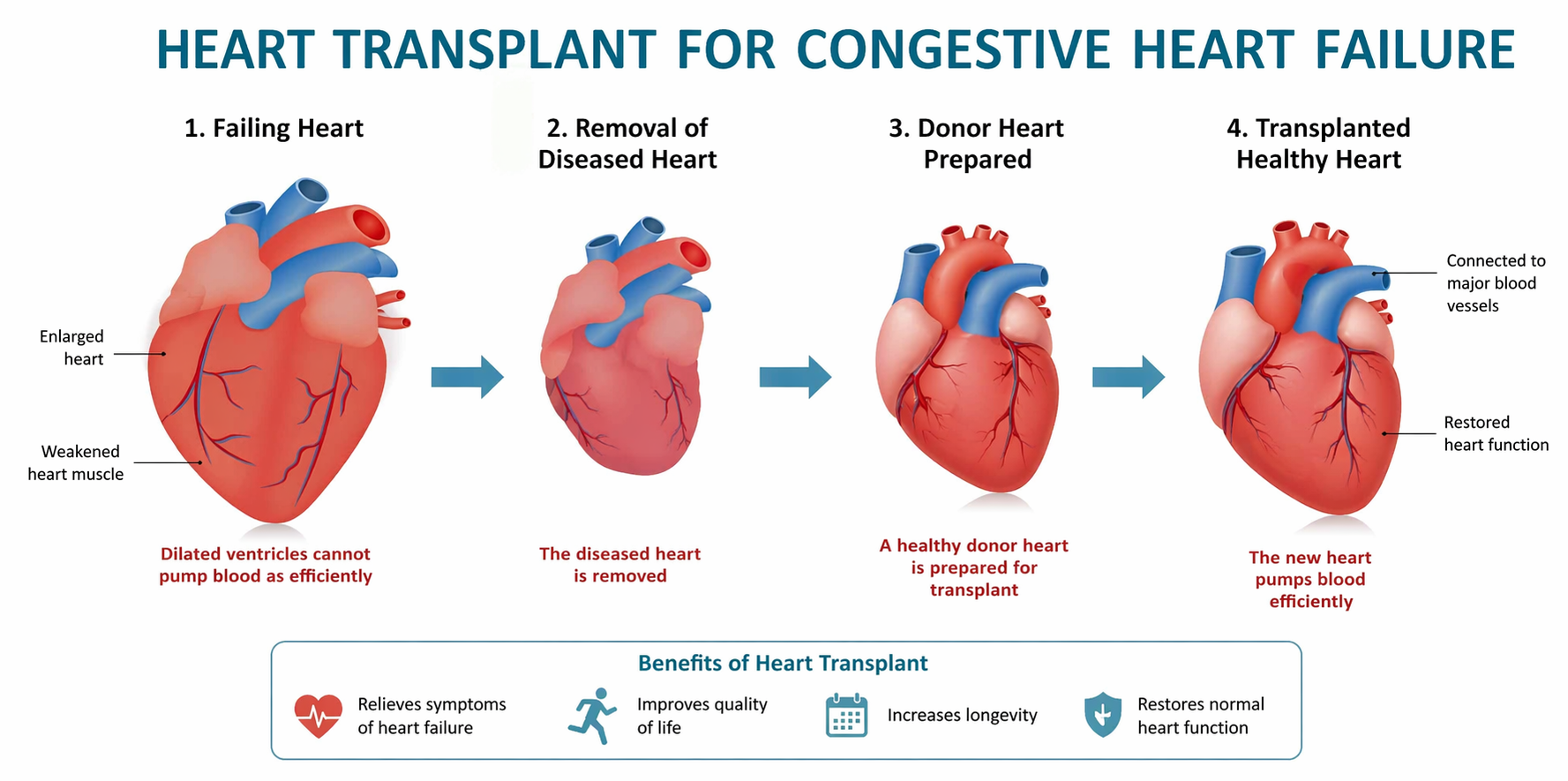
A heart transplant for congestive heart failure is a surgical procedure in which a patient’s failing heart is replaced with a healthy donor heart. It becomes necessary in end-stage (Stage D) heart failure when medications, devices, and other surgeries stop working, and ejection fraction and overall cardiac function keep declining.
“We don’t rush transplants. By the time we’re even suggesting one, we’ve usually tried everything else first. Timing really is most of the battle.” — Cardiac Surgeon in Mumbai, Dr. Vishal Khullar
Heart failure almost never presents in a single dramatic moment. It builds. Someone notices stairs feel a bit harder this month than last. Ankles are getting puffy at night. Sleeping sat up because flat just feels wrong somehow. Medicines help, sure, but eventually less so. Then one day the conversation shifts from adjusting doses to something much bigger: the possibility of replacing the heart itself.
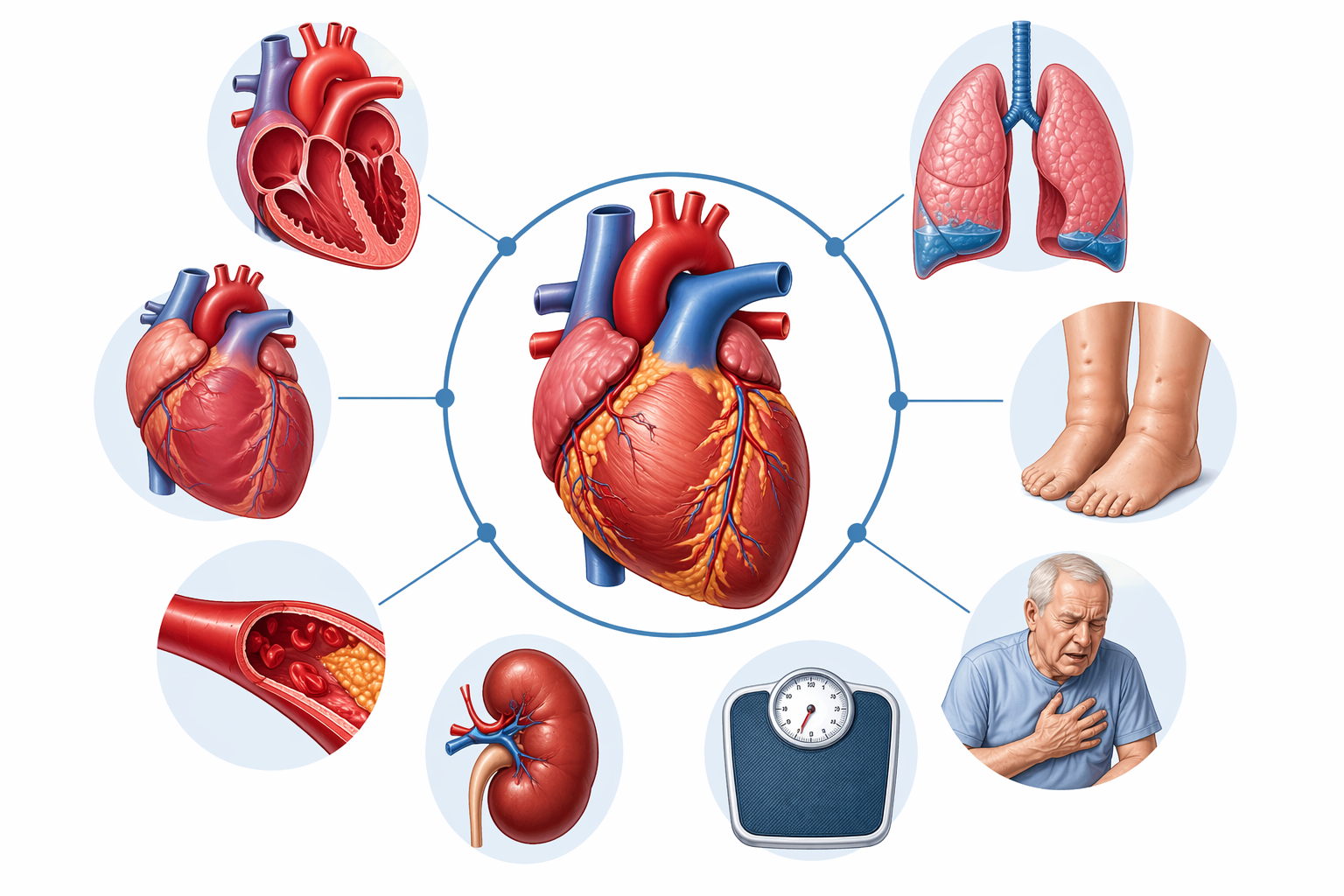
A simple way to put it: the heart can’t pump enough blood around for what the body actually needs. It hasn’t stopped, just tired. Blood backs up, fluid sneaks into the lungs (that’s the breathlessness part), and it pools in the legs and belly. Kidneys, sensing reduced flow, begin to retain salt and water. Everything gets puffy, everything feels heavier.
CHF has four stages, A through D. Early on, medicines do most of the work: diuretics, beta-blockers, ACE inhibitors, and the newer SGLT2 inhibitors, with a pacemaker, ICD, or CRT added in if rhythm is the problem. Most patients do all right for years on that combination, and it’s Stage D where things stop adding up. Worth noting, some patients still early enough in the disease respond beautifully to heart bypass surgery, which can push transplant off the table entirely for a long time.
Book a consultation with Dr. Vishal Khullar to understand your heart condition before it progresses into end-stage heart failure.
It becomes necessary once CHF hits the end stage. Maximum medical therapy, lifestyle changes, devices, none of it is doing the job anymore. Transplant isn’t an early move; it’s the door that opens once everything else has shut.
By this point, symptoms are loud, not subtle. They show up together and keep getting worse, no matter how the medications are adjusted.
When two or more of these keep getting worse despite every adjustment, that’s the moment to refer for transplant evaluation..
Not every patient with severe CHF qualifies, and there’s a reason. A new heart needs a body strong enough to survive major surgery and handle lifelong immunosuppression afterward.
Generally eligible if:
Things that rule it out:
The list isn’t flexible. For patients not ready right now, an LVAD – Left Ventricular Assist Device can either bridge them to transplant later or work as a standalone long-term therapy.
Consult Dr. Vishal Khullar to check your eligibility and explore advanced heart failure treatment options.
This is a process, not just an operation. Starts months before surgery, doesn’t really end.
Complete workup before anyone gets listed. ECG, echo, cardiac catheterization, right heart catheterization to measure pulmonary pressures, blood and tissue typing, lung function, kidney and liver panels, cancer screening, psychological evaluation. The whole point of this stage is figuring out whether a transplant is genuinely the right call.
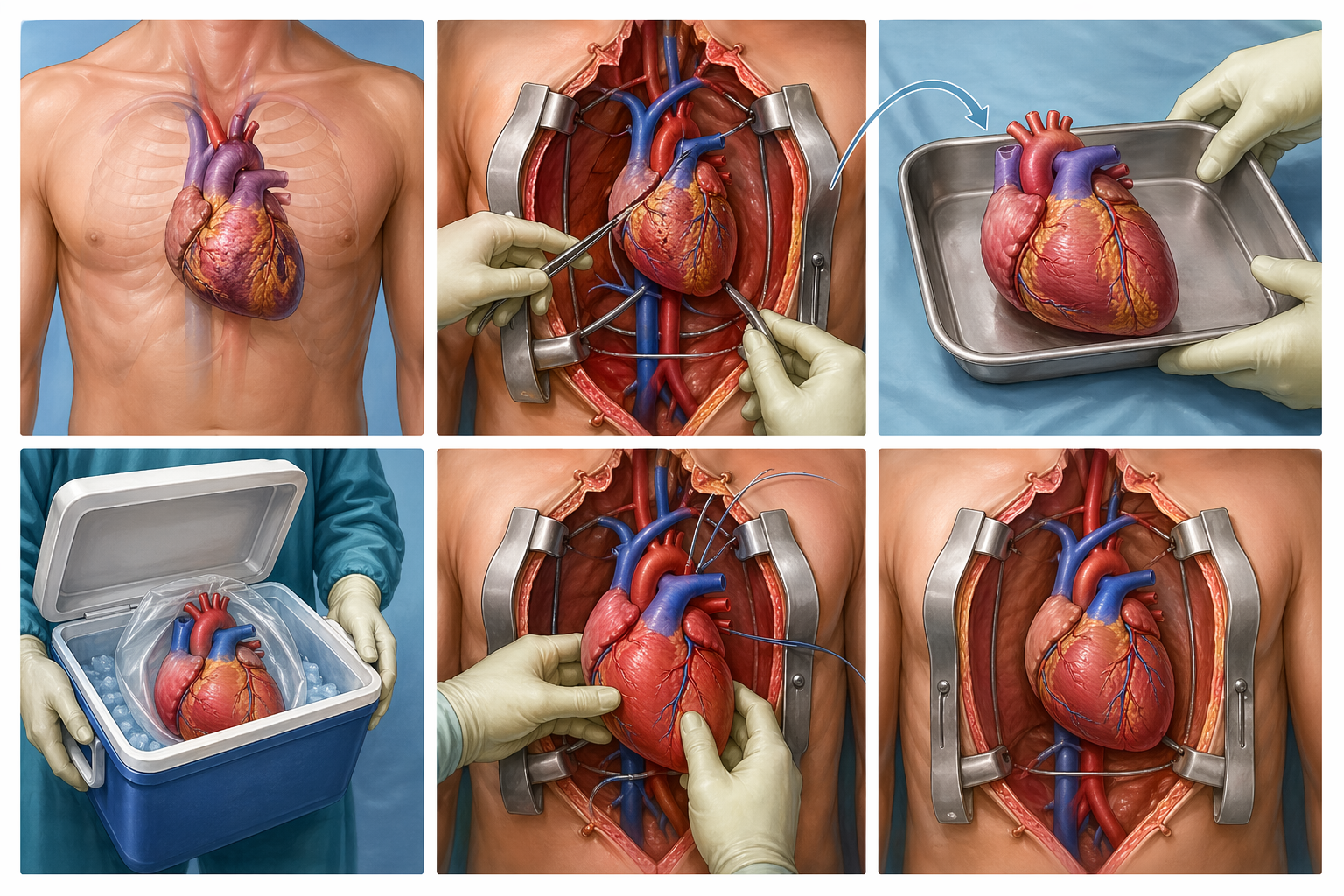
Once cleared, the patient is added to the list. Matching runs on blood group, body size, and immune profile. Waiting time depends entirely on donor availability, which can mean weeks or many months.
Four to six hours, usually. The diseased heart comes out. The donor heart goes in, connected to the major vessels. Blood flow restored, the new heart starts beating on its own. That moment still feels remarkable every single time, even after 300 transplants.
ICU stage is all about watching three things: rejection, infection, and hemodynamic stability. Immunosuppressants begin immediately. Rehab builds up slowly once the patient’s clearly stable.
Any major surgery carries risks, this one included. Rejection is the biggest, which is why immunosuppressants never stop. Infection risk stays elevated because immunity is deliberately suppressed. Long-term medication can strain the kidneys, push blood pressure up, or bring on diabetes. Cardiac allograft vasculopathy, a gradual narrowing of the donor heart’s arteries, is something to watch over the years. Bleeding, arrhythmias, early post-op stuff, standard parts of the recovery window.
None of this is a reason to skip transplant when it’s truly needed. It’s just a reason to pick the surgeon and center carefully. Really carefully.

Dr. Vishal Khullar’s supreme expertise and dedication make him the premier choice for heart transplant and end-stage heart failure treatment in Mumbai. His commitment to excellence ensures that patients receive the highest level of care and the best possible outcomes.
Heart transplant for congestive heart failure saves lives when everything else has been tried. Not a last-minute decision, though. It’s a carefully timed one, made together by patient, family, and a surgical team that understands both the disease and the person living with it. Timing being such a big deal means the surgeon evaluating you matters as much as the operation itself. Refer early. Options stay open that way.




