Trusted By
9,000+ Patients Globally
Mitral valve prolapse occurs in 1 out of 40 individuals; therefore, it’s a very common thing within the realm of heart surgery. Some people live with mitral valve prolapse all their lives without any symptoms, but the ability to distinguish when heart surgery really needs to occur could make a world of difference. Otherwise, you could very well let a simple heart procedure turn into a rather big deal.
When it comes to having surgery for my mitral valve prolapse, it basically depends on several factors, and those are the severity of my mitral regurgitation, the status of my left ventricle, my symptoms, and whether my valve can be repaired. Follow-up visits with my cardiac surgeon and other diagnostic tools, such as echocardiograms, TEE, and cardiac MRI, allow us to monitor my condition. Yet, sometimes it’s that weird sound that my stethoscope exam reveals, which gives me the first sign that something’s not quite right.
Dr. Vishal Khullar, as an experienced cardiac surgeon in Mumbai, has observed that those patients who find the right time to undergo the surgery generally fare much better than those who wait until their hearts are already damaged. The choice to undergo the surgery involves evaluating personal risk factors and how effectively the heart is functioning. For this reason, the American Heart Association urges seeking the advice of an expert when the severity of the valve disease is on the rise.

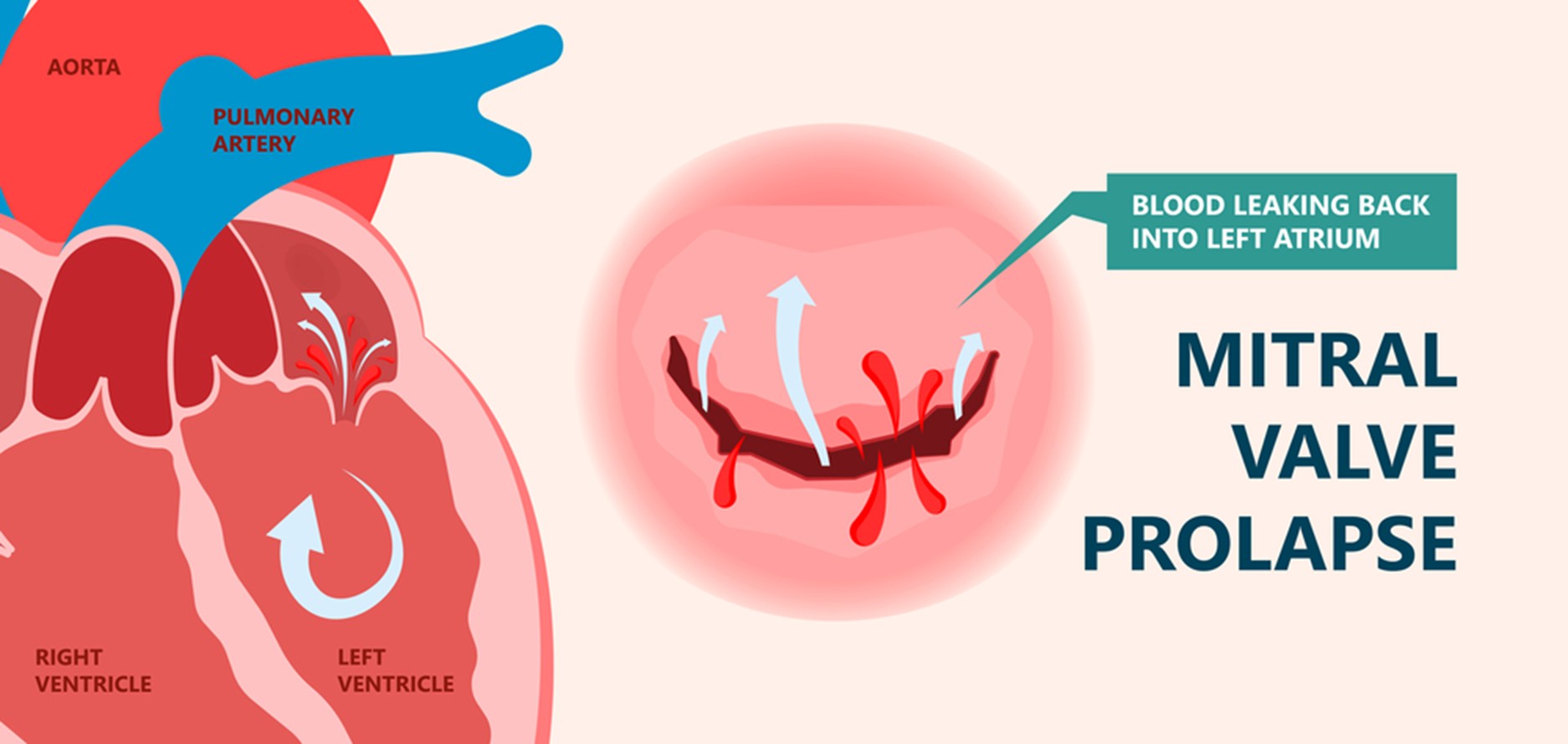
Mitral Valve Prolapse (MVP), also known as “floppy valve syndrome” and “click-murmur syndrome,” occurs when the flaps between the left atrium and ventricle do not close properly. Instead of meeting in a tight seal, the flaps prolapse back up into the atrium during a heartbeat cycle.
Normally, it would open to allow blood to pass through from the atrium to the ventricle and then close to prevent backflow. The chordae tendineae and muscles of supply, or the actual flaps, may weaken or stretch, causing the flaps to be floppy and unable to close properly. And that is when you can get mitral regurgitation (MR)–blood leakage into the atrium. Mitral regurgitation does not cause problems when it is mild, but severe mitral regurgitation forces the heart to work extra hard because of the reduced flow.
Over months to years, this additional work may cause the left atrium and ventricle to stretch. The heart muscle may begin to weaken, and the pumping action becomes less effective. All the way from slight prolapse and minimal leakage to chordae snapping or the flail leaflet having no support whatsoever, we see the whole spectrum. A lot or a little mitral valve regurgitation, trust me, it really does impact heart function. Most people with MVP don’t even realize it, but when severe MR kicks in, the heart is going to start to remodel, and it is very hard to reverse. This is why it is so relevant to understand MVP and its impact on the heart when considering surgery.
We watch for a few potential indicators that surgery may be required for a mitral valve prolapse. Most people will never require a surgical procedure, but there are some symptoms or test results that dictate that the time has come to have one.
The usual vessels we use for grafting are:
When these symptoms appear, it can be known that the valve is leaking quite a lot. The heart has to work harder, and eventually, the ventricles can become stretched and weakened.
Conditions like atrial fibrillation, and even sudden episodes of racing heart, give us a hint that the heart’s electrical system is becoming unsettled, and may increase your risk for stroke. We also look for signs that you may be having heart failure, like swelling in the legs, and very difficult breathing.
There’s also the importance of diagnostic tests. Even if you’re feeling perfectly healthy, if your echocardiogram indicates severe regurgitation, you could potentially require surgery. An enlarged heart or an indicator of declining ejection fraction—the value of the contraction of the heart, its pumping power—is a significant warning sign.
It’s not always easy. Sometimes people can have no symptoms at all and yet have seriously dysfunctional valves on imaging studies. Or they can be symptomatic and have not too bad valves. That’s why only a full workup can tell a doctor when surgery is indicated.
If you’re experiencing breathlessness, fatigue, or irregular heartbeats, schedule a detailed heart valve evaluation with Dr. Vishal Khullar today.
If you delay surgery when mitral valve prolapse progresses to severe mitral regurgitation, you might end up with permanent heart problems. We’ve seen some people who waited for too long and developed left ventricular dysfunction. Even after surgery, their prognosis is not so favorable.
The biggest risk factor for waiting is heart failure. As the blood keeps seeping back, the left ventricle keeps working overtime. The heart literally becomes unable to keep up. Its ejection fraction declines, and everything spirals out of control.
On the other hand, patients who undergo surgery for mitral valve prolapse at the appropriate time usually recover heart function well enough that their long-term outlook is often comparable to that of people without heart disease. In contrast, delayed treatment can allow permanent damage to the heart or lungs, which may limit recovery even after surgery and affect overall quality of life.
Symptoms of mitral valve prolapse tend to progress indolently, and it is thus easy to ignore them as the heart silently remodels. High-risk patterns, such as mitral annular disjunction, have a risk of arrhythmias and may persist once surgery is delayed. Acting before irreversible changes occur offers the best chance for normal heart function and long-term cardiac health.
People with mitral valve prolapse do much better when surgeons intervene at just the right time, compared with those who delay treatment. Early mitral valve repair helps keep the left ventricle working well and prevents permanent heart muscle damage that can sneak up if severe regurgitation drags on for too long.
When surgery happens sooner, it’s usually simpler to repair the mitral valve instead of having to replace it with a mechanical one.
Going in for surgery before the heart gets too worn out means patients face a lower risk during the operation.
Research shows that getting the timing right can give patients survival rates close to those without heart issues.
If the surgeon can repair the valve, patients can usually skip lifelong blood thinners, which are necessary with a mechanical valve.
Acting early helps prevent atrial fibrillation, heart failure, and pulmonary hypertension from developing down the road.
Patients undergoing mitral valve prolapse surgery before heart enlargement generally heal more quickly and retain their heart function better. Present methods for less invasive surgery heal more quickly than conventional surgery, and surgical repair featuring an annuloplasty ring returns normal support to the valve. While medications such as beta blockers or diuretics are available to alleviate symptoms, they would not repair the actual problem with the valve. Letting the problem progress could lower the chances for repair and raise the requirements for valve replacement.
If you’ve been diagnosed with mitral valve prolapse or advised surgery, consult Dr. Vishal Khullar to assess the right timing for long-term heart health.