Trusted By
9,000+ Patients Globally
Heart bypass surgery in patients under 40 is no longer rare in India. Roughly one in four heart attacks now happens in people below 40, and around 10 to 13 percent of these young patients need coronary artery bypass grafting (CABG) instead of just a stent. The main drivers are family history, diabetes, high LDL cholesterol, smoking, undiagnosed high blood pressure, and an urban lifestyle. With the right surgeon, the 5-year survival after CABG in young Indians sits at around 91.8 percent.
Dr. Vishal Khullar, an experienced Cardiac Surgeon in Mumbai, India, trained at Mayo Clinic and Cleveland Clinic, and currently the Director of the heart and lung transplant program at Fortis Mulund, has operated on hundreds of patients in their twenties, thirties, and early forties. This blog explains why young Indians are showing up with severe coronary artery disease this early, when bypass surgery is the right call, and what recovery actually looks like.
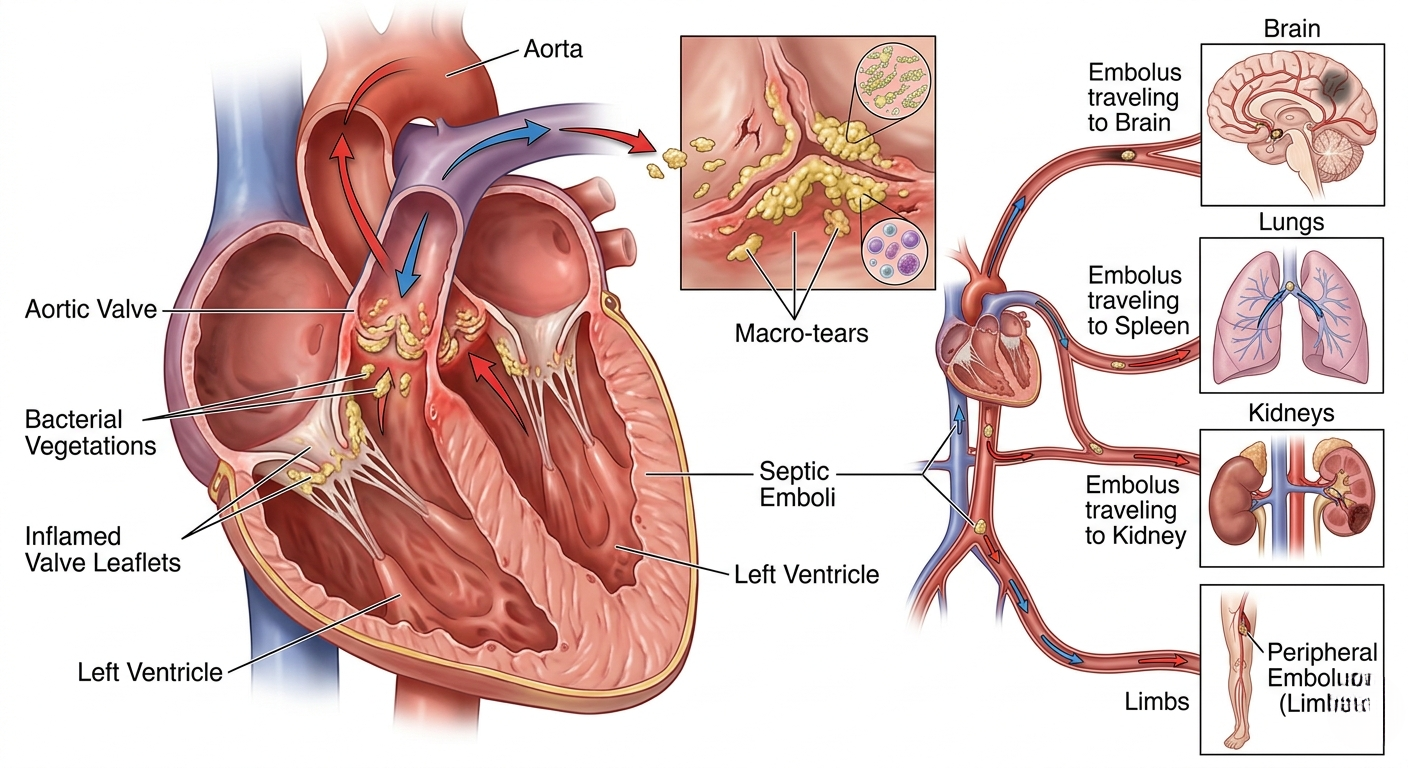
Bacteria, and occasionally fungi, settle on a heart valve and form clumps called vegetations. These damage the leaflets, can chew through them entirely, and can break off to travel to the brain, lungs, kidneys, or limbs. The valve fails, the heart starts to fail, and the infection keeps seeding new sites. Some patients respond to six weeks of intravenous antibiotics; others don’t. When the valve is being destroyed in real time, infective endocarditis surgery is the only intervention that stops the disease.
Book a consultation with Dr. Vishal Khullar to understand whether your case needs surgery or can be managed with antibiotics.
If any of the following are present, surgery is usually the treatment, not an option:
Endocarditis surgery depends on which valve is affected and, crucially, how far the infection has spread beyond it. The surgeon’s job is always the same: remove every last bit of infected tissue, then rebuild what the infection destroyed. The most common reason endocarditis recurs after surgery is that infected tissue was left behind, so a complete operation matters more than a quick one.

When infection spreads past the aortic valve leaflets into the aortic root, it forms an abscess, a pocket of infected, dead tissue around the base of the aorta. Simply replacing the valve and leaving that abscess behind is not a complete solution. The infection sits in the root, keeps eating through tissue, and comes straight back, often within weeks, on the brand-new valve.
The correct operation is a full aortic root replacement. The entire infected root is removed, the valve, the diseased aortic wall and the abscess cavity, leaving only clean tissue. The coronary arteries are detached and reimplanted, and the root is rebuilt with a homograft (a human donor aortic root) or a valved conduit; in active infection a homograft is often preferred because biological tissue resists reinfection far better than artificial material. It is a much bigger operation than a valve swap, but when the root is involved it is the only one that actually cures the disease.
The hardest cases are those where infection has destroyed both the aortic and mitral valves along with the tissue between them, the aorto-mitral curtain (intervalvular fibrous body). This fibrous bridge anchors both valves. Once infection eats through it, replacing the valves alone is pointless, because there is no solid foundation to sew them onto.
The commando operation answers this and is one of the most demanding procedures in cardiac surgery. The surgeon removes both infected valves, debrides the destroyed curtain completely, reconstructs it with a patch (pericardium or Dacron), then implants new aortic and mitral valves onto that rebuilt base; the roof of the left atrium often has to be reconstructed too. The hemi-commando is a less extensive version used when the aortic valve and curtain are involved but the mitral valve can still be saved, the choice depending on how much of the mitral valve the infection has destroyed.
Both carry higher risk than standard valve replacement, but in experienced hands they are the difference between curing extensive infection and watching it recur on fresh valves. Dr. Khullar performs these aorto-mitral reconstructions, including commando and hemi-commando procedures, for the most advanced cases. Where leaflets are salvageable, repair is preferred; when replacement is needed, the mechanical-versus-tissue choice is explained in this guide to mechanical vs tissue heart valves by age.
![P]009](https://drvishalkhullar.com/wp-content/uploads/p009.png)
These patients are usually very sick; many are septic and some have already had a stroke. The family deserves an honest picture:
Operating early, before multi-organ failure, dramatically improves outcomes; operating late, after a major stroke or septic shock, makes everything harder.
Recovery starts with two to four days in ICU and five to seven on the ward. IV antibiotics continue for four to six weeks total, and cardiac rehab begins within two to three weeks. Most patients return to a near-normal routine within three months.
The decision to operate, and exactly when, is often more important than the surgery itself. Operate too early and you expose a patient to unnecessary risk; wait too long and the infection eats through the valve, throws an embolus, or causes septic shock. Dr. Vishal Khullar’s training at Mayo Clinic and Cleveland Clinic and his experience with hundreds of cases at Fortis Mulund make a real difference at this decision point.
Book an appointment with Dr. Vishal Khullar to discuss surgery, timing, and the best path forward.