Trusted By
9,000+ Patients Globally
When a patient is told they need a heart transplant, the first question is almost never about the surgery. It is about the wait. How long will it take? Will the heart hold on? What happens in the meantime?
These are not abstract concerns. Donor hearts are scarce, waiting lists are real, and the heart that needs replacing is already struggling. For many patients, the body simply cannot hold on without some form of help during that period.
Dr. Vishal Khullar, an experienced Cardiac Surgeon in Mumbai trained at Mayo Clinic and Cleveland Clinic, currently the Director of heart and lung transplant program at Fortis Hospital, Mulund, has worked with some of the most critically ill heart failure patients in India and the United States. This blog draws on that experience to explain what mechanical circulatory support actually is, how it keeps patients alive during the transplant wait, and what that period genuinely looks like for patients and their families.
It is one of those medical phrases that gets used often but is rarely explained properly. A bridge to transplant simply means using a mechanical device to keep a critically ill patient alive and stable while they wait for a donor heart.
Without this support, a significant number of these patients would not survive long enough to receive the transplant they need. Their hearts are too weak. Their organs are already under strain. The medications that once helped have run their course.

It is one of those medical phrases that gets used often but is rarely explained properly. A bridge to transplant simply means using a mechanical device to keep a critically ill patient alive and stable while they wait for a donor heart.
Without this support, a significant number of these patients would not survive long enough to receive the transplant they need. Their hearts are too weak. Their organs are already under strain. The medications that once helped have run their course.
That last point matters more than people realise. A patient who is well enough to go home, stay mobile, and maintain some quality of life during the wait is in a far better position to recover from transplant surgery than one who has been deteriorating in a hospital bed for months.
Facing a heart transplant wait? Speak with Dr. Vishal Khullar about your support options.
Not every device is right for every patient. The choice depends on how sick the patient is, how suddenly the heart has deteriorated, which part of the heart is failing, and what the surgeon assesses as the most stable path forward.
ECMO is brought in when both the heart and lungs are failing, and the patient needs support immediately. The machine takes over the work of both organs from outside the body, keeping blood circulating and oxygenated while the team stabilises the patient and works out what comes next.
It is not a long-term solution. ECMO buys days to weeks, not months. It is used in the most acute and urgent situations — sudden collapse, cardiogenic shock, rapid deterioration — and it is almost always a bridge to something else. That next step might be an LVAD, a transplant, or in some cases a conversation about what is realistic.
An LVAD is a pump surgically placed inside the chest that takes over the pumping work of the left ventricle. It is built for medium to long-term use — months, and sometimes years.
For patients who are listed for a transplant but too sick to survive the wait without help, an LVAD is often the most appropriate choice. It gives many patients the ability to leave hospital, return to some level of daily function, and wait in a far more dignified and stable condition. When the donor heart eventually becomes available, the LVAD is removed and the transplant is performed.
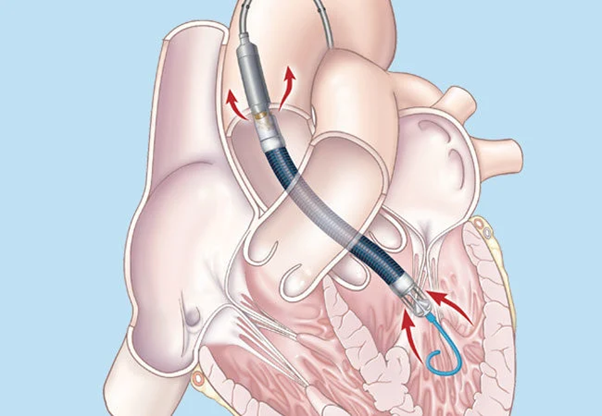
An intra-aortic balloon pump is a less invasive device inserted through the groin that inflates and deflates in rhythm with the heart to reduce the load on the left ventricle. It is used when a patient is deteriorating but has not yet reached full cardiac collapse — buying a window of time for the team to make a considered decision about what support is needed next.
It plays a specific and valuable role but is not typically the device that carries a patient through a long transplant wait.
There is no formula for this. It is one of the most nuanced judgment calls in all of cardiac surgery, and it requires weighing several things at the same time.
In some patients, the journey involves more than one device. A patient may arrive in cardiogenic shock, be placed on ECMO as an emergency measure, be stabilised enough for LVAD implantation over the following days, and eventually receive a transplant several months later. Surgeons sometimes call this a staged bridging approach and it requires careful coordination across the entire cardiac team.
Every MCS decision is unique. Get an expert opinion from Dr. Vishal Khullar.
This is what families want to know and rarely get a straight answer on. When the heart fails severely, every organ in the body begins to suffer because it is not receiving enough oxygenated blood. The kidneys struggle. The liver is under strain. The patient feels exhausted, breathless, and often confused about why they feel so unwell even when they are not in obvious pain.One of the most important things mechanical circulatory support does is begin to reverse that process.
This organ recovery is not just about how the patient feels day to day. It is clinically critical. A patient whose kidneys and liver have had time to recover during the bridging period is significantly more likely to survive transplant surgery and recover well from it than a patient whose organs were already damaged at the point of transplant.
Mechanical circulatory support saves lives. It also carries real risks, and patients and families deserve to understand those clearly before any decisions are made.
These risks are real but they are managed through careful patient selection, experienced surgical technique, and close ongoing follow-up. In almost every case where mechanical support is recommended for a transplant candidate, the risk of not using it is considerably greater than the risk of using it.
According to the International Society for Heart and Lung Transplantation, patients who are well managed on mechanical circulatory support before transplant have long-term outcomes comparable to those who went directly to transplant without prior mechanical support.

The transplant wait is one of the most emotionally demanding periods a patient and family can go through. Knowing what to expect practically does not make it easy, but it does make it less frightening.
The emotional weight of this period should not be underestimated. Dr. Khullar’s team works closely with patients and families throughout the bridging period, making sure that nobody faces the uncertainty of that wait without clear communication and proper support around them.
Waiting for a heart transplant is never easy. But for patients whose hearts cannot hold on through that wait without help, mechanical circulatory support is not a last resort. It is a carefully considered strategy — one that keeps the body alive, gives vital organs a chance to recover, and ensures that when the transplant does happen, the patient is in the best possible position to benefit from it.
The difference between a good outcome and a poor one often comes down to two things — how early that conversation starts, and how experienced the team having it is.
Advanced heart failure needs advanced expertise. Book your consultation in Mumbai today.