Trusted By
9,000+ Patients Globally
Surgeon: Dr. Vishal Khullar | Specialty: Cardiothoracic & Vascular Surgery, Heart and Lung Transplant
Hospital: Nanavati Max Super Speciality Hospital, Vile Parle West, Mumbai
Procedure: Coronary Artery Bypass Grafting using Bilateral Internal Thoracic Arteries and Left Radial Artery Conduit
Video Testimonial: youtu.be/kyfas1psgro
Patient details below have been recorded in line with confidentiality conventions for written case studies. The patient has separately provided consent for an on-camera testimonial published on Dr. Khullar’s official channel, which is linked in Section 09a.
|
Age |
52 years |
|
Gender |
Male |
|
Occupation |
Working Professional |
|
Residence |
Resident of Dubai, treated in Mumbai |
|
Presenting Complaint |
Chest pain and breathlessness on exertion |
|
Diagnosis |
Critical triple vessel coronary artery disease with reduced left ventricular function |
|
Duration of Issue |
Approximately 1.5 years (post prior cardiac event) |
|
Co-morbidities |
Type 2 Diabetes Mellitus, Hypertension |
|
Previous History |
Previous myocardial infarction roughly 1.5 years prior |
|
Date of Procedure |
Confirmed admission and surgery (per clinical record) |
|
Outcome |
Successful — uneventful recovery |
Condition
The patient presented with chest discomfort on exertion and reduced exercise tolerance. Clinical evaluation pointed toward advanced coronary disease in a heart already weakened by an earlier infarction. Echocardiography confirmed a left ventricular ejection fraction of 30 percent, indicating significantly reduced pumping efficiency. Coronary angiography revealed critical narrowing across all three major coronary territories, classified as triple vessel disease. The condition was severe and warranted urgent surgical intervention through heart bypass surgery to restore coronary perfusion and protect the remaining myocardium.
Impact on the Patient
The patient had been managing two long-standing chronic conditions, diabetes and hypertension, both of which independently raise cardiac risk. After his previous heart attack, daily life had become measured by what activity he could tolerate. Travel from Dubai to Mumbai for definitive treatment was prompted by worsening symptoms and the recognition that medical therapy alone would no longer suffice. By the time he reached our outpatient clinic, even ordinary exertion was producing chest discomfort. The clinical picture was time sensitive, and the family arrived seeking a surgical team experienced in high risk coronary cases.
What Was Assessed During the Consultation
Why This Surgical Approach Was Chosen
Pre-operative documentation included resting echocardiography, coronary angiography, baseline biochemistry with HbA1c, and standard cardiac surgical workup. Imaging confirmed the surgical plan and the choice of conduits.
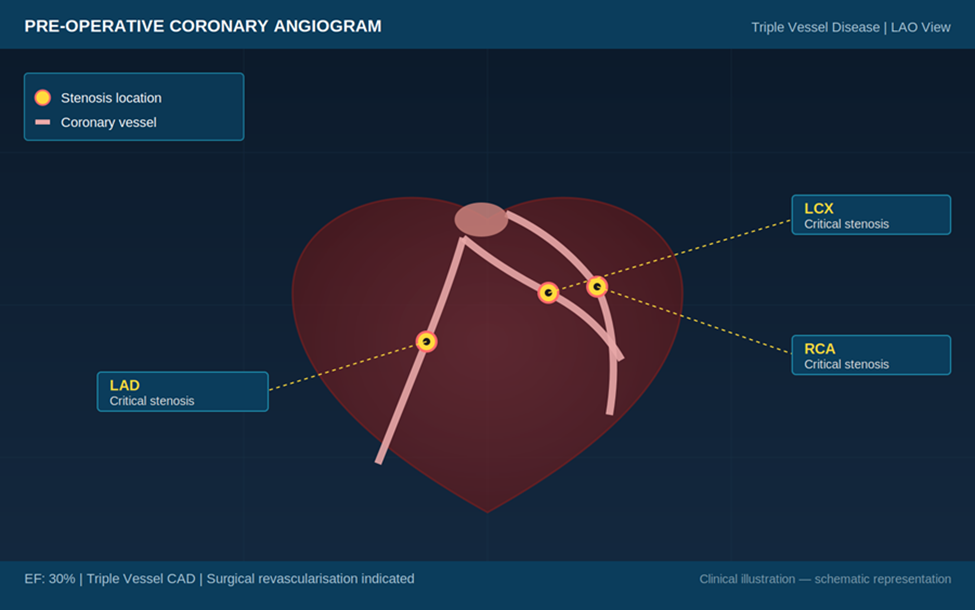
Figure 1. Pre-operative coronary angiogram — schematic representation of triple vessel disease across the LAD, LCX, and RCA territories
Figure 1. Pre-operative coronary angiogram — schematic representation of triple vessel disease across the LAD, LCX, and RCA territories
Step-by-Step Surgical Overview
The choice of complete arterial revascularisation reflects Dr. Khullar’s training at Mayo Clinic and Cleveland Clinic in the United States, where multi-arterial conduit strategies are standard for younger patients and patients with diabetes.
Procedure Facts
|
Procedure |
Coronary Artery Bypass Grafting (Triple Vessel) |
|
Anaesthesia |
General anaesthesia with cardiac specific protocol |
|
Conduits Used |
Bilateral Internal Thoracic Arteries plus Left Radial Artery |
|
Approach |
Median sternotomy with cardiopulmonary bypass |
|
Special Considerations |
Pre-operative ejection fraction 30 percent; diabetic patient |
|
Intra-operative Course |
Stable; no adverse events recorded |
|
Total Theatre Time |
Within standard duration for triple vessel arterial revascularisation |
|
Hospital Stay |
Discharged on post operative day 5 |
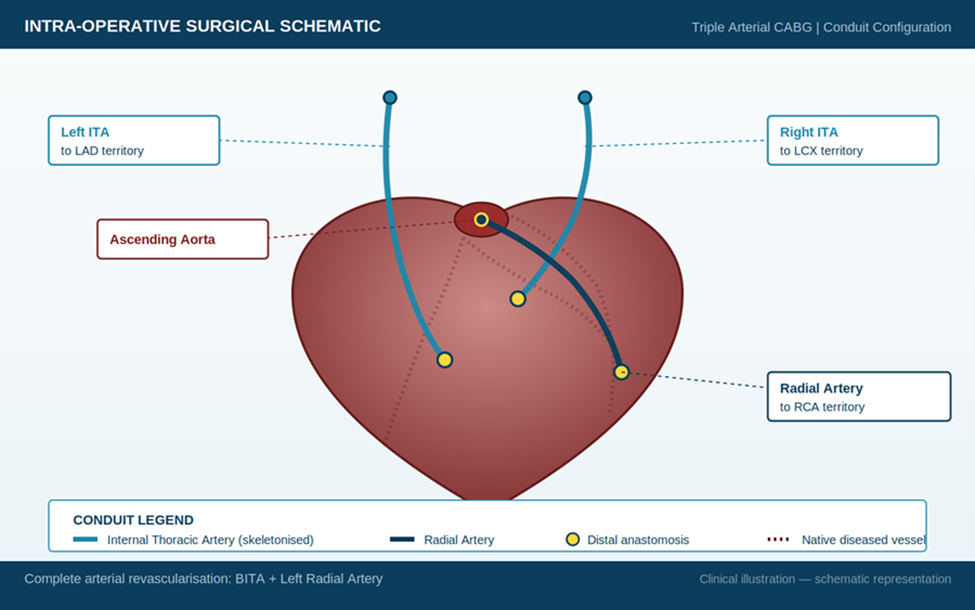
Figure 3. Intra-operative surgical schematic — complete arterial revascularisation using bilateral internal thoracic arteries and the left radial artery conduit
Recovery progressed in line with the surgical plan. The patient was extubated on post operative day 1 and discharged on post operative day 5. Symptom relief was reported early in the recovery phase, and clinical observation at follow up confirmed restored exercise tolerance with no recurrence of angina. Glycaemic control and blood pressure were stabilised within the recovery period.
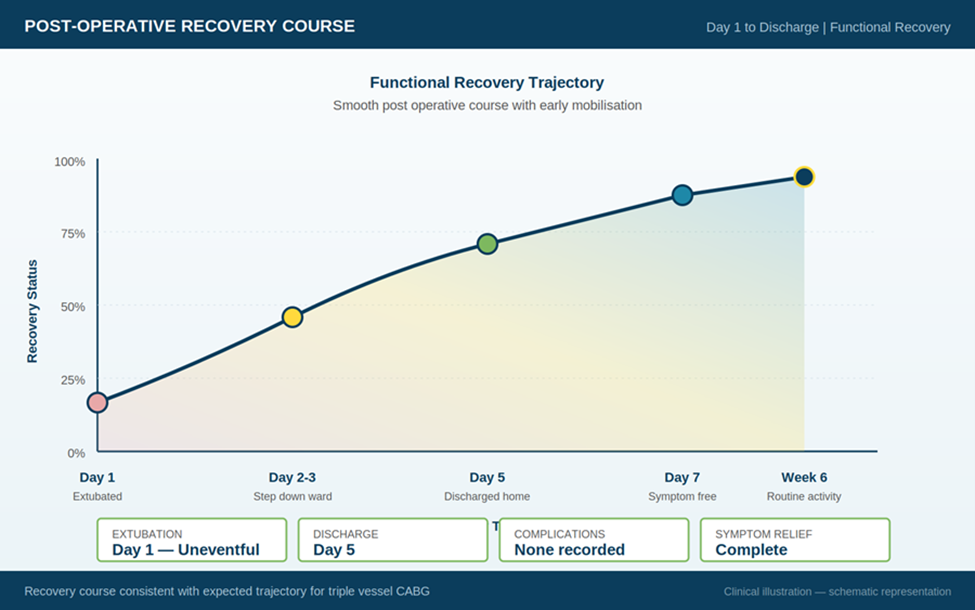
Figure 4. Post-operative functional recovery trajectory — uneventful course from extubation through discharge and return to routine activity
Outcomes at a Glance
|
Outcome Metric |
Result |
|
Revascularisation |
Complete arterial revascularisation across all three target vessels |
|
Extubation |
Day 1 post-operative — uneventful |
|
Discharge |
Day 5 post-operative |
|
Symptom Relief |
Resolution of exertional chest pain and breathlessness |
|
Complications |
None recorded during admission |
|
Recovery Course |
Smooth — within expected clinical timeline |
|
Patient Reported Outcome |
Returned to normal activity within roughly seven days at home |
Recorded during clinical follow up. Quotation reflects the patient’s own words.
|
I had travelled from Dubai to Mumbai because my condition had become critical. I am a diabetic patient and had a previous cardiac event some time before. When Dr. Khullar reviewed my reports, the situation was serious. The surgery was carried out and the recovery went well. Within seven days I felt healthy again. The doctor and the entire hospital staff looked after me thoroughly. I am grateful to Dr. Khullar and to Nanavati Max Hospital for the care provided. Patient profile: Male · 52 years · Working Professional · Resident of Dubai Procedure: Triple Vessel CABG · Nanavati Max Super Speciality Hospital, Mumbai Surgeon: Dr. Vishal Khullar · Director, Cardiothoracic & Vascular Surgery, Heart and Lung Transplant |
More patient experiences are available on the patient testimonials page.
The same patient and the operating surgeon are featured in an on-camera testimonial published on Dr. Vishal Khullar’s official YouTube channel. The video records the patient’s clinical history, the surgeon’s account of the operative decision, and the patient’s recovery in his own words. Click the thumbnail below or use the link to watch.
Video Title: Successful Bypass Surgery for Severe Coronary Blockages — Patient Testimonial featuring Dr. Vishal Khullar
Channel: Dr. Vishal Khullar (Official)
Featured Voices: The patient, and Dr. Vishal Khullar, Director, Cardiothoracic and Vascular Surgery, Nanavati Max Super Speciality Hospital, Mumbai
Instructions Provided to the Patient
Recovery Timeline
|
Timeframe |
Clinical Expectation |
|
Day 1 |
Extubated; transferred to cardiac care unit; haemodynamics monitored |
|
Day 2 to 4 |
Step down ward; mobilisation begins; glycaemic and pain protocols active |
|
Day 5 |
Discharge home with detailed care instructions and medication chart |
|
Week 1 to 2 |
Light activity at home; sternal precautions; first follow up review |
|
Week 6 |
Return to normal day to day activity; sternal healing assessed |
|
Month 3 |
Cardiac rehabilitation review; exercise tolerance reassessed |
|
Month 6 to 12 |
Long term follow up; graft patency confirmed clinically; medication optimisation |
Q.1 Why is bypass surgery preferred over stenting for triple vessel coronary disease in a diabetic patient with reduced heart function?
Long term studies have consistently shown that surgical revascularisation provides better survival and lower rates of repeat intervention in diabetic patients with disease across all three coronary territories, particularly when the heart’s pumping function is reduced. Read more about heart bypass surgery in Mumbai performed by Dr. Vishal Khullar at Nanavati Max Super Speciality Hospital.
Q.2 What is the advantage of using bilateral internal thoracic arteries and the radial artery during CABG?
Arterial grafts remain open longer than vein grafts over decades of follow up. Using two internal thoracic arteries from the chest wall together with a radial artery from the forearm provides complete arterial revascularisation, which lowers the long term need for further coronary interventions. This approach is well suited to younger patients and to those with diabetes.
Q.3 How long does recovery take after triple vessel bypass surgery?
Most patients are extubated within twenty four hours, transferred out of intensive care within two to three days, and discharged home around day five to day seven. Light home activity resumes during the first two weeks, and routine work and travel are usually possible by six weeks. The sternum takes around six to eight weeks to heal.
Q.4 Is heart bypass surgery safe in a patient who already has a low ejection fraction and diabetes?
Outcomes in such patients depend heavily on surgical planning, anaesthetic management, and perioperative care. With experienced teams and modern techniques, including arterial conduits and protective bypass strategies, results in high risk patients have improved substantially. Learn more about Dr. Vishal Khullar, whose training at Mayo Clinic and Cleveland Clinic informs his structured approach to high risk coronary cases.
Q.5 Why do international patients travel to Mumbai for cardiac surgery?
Mumbai offers a combination of internationally trained cardiac surgeons, modern hospital infrastructure, and cost effective comprehensive care. International patients can contact the clinic directly to discuss travel arrangements, second opinions, and pre-arrival cardiac workup.
Q.6 Where can I watch this patient’s full testimonial?
The patient’s full on-camera testimonial, along with Dr. Vishal Khullar’s clinical summary, is published on the surgeon’s official YouTube channel at youtu.be/kyfas1psgro. The recording covers the patient’s history, the surgical plan, and his recovery in his own words.