Trusted By
9,000+ Patients Globally
Surgeon: Dr. Vishal Khullar | Specialty: Cardiothoracic & Vascular Surgery, Heart and Lung Transplant
Hospital: Nanavati Max Super Speciality Hospital, Vile Parle West, Mumbai
Procedure: Redo Mitral Valve Replacement with Coronary Artery Bypass Grafting
Video Testimonial: youtu.be/kyfas1psgro
|
Age |
61 years |
|
Gender |
Female |
|
Occupation |
Homemaker |
|
City |
Thane, Maharashtra |
|
Presenting complaint |
Breathlessness on exertion and chest pain |
|
Diagnosis |
Degenerated mitral bioprosthesis (failed tissue valve) with coexisting coronary artery disease |
|
Duration of issue |
Symptoms developed roughly three to four years after the original valve replacement |
|
Previous treatment |
Prior mitral valve replacement using a tissue (bioprosthetic) valve |
|
Date of procedure |
May 2025 |
|
Outcome |
Excellent symptom-free since surgery |
The condition
The patient had previously undergone mitral valve replacement with a tissue (bioprosthetic) valve. Unlike mechanical valves, bioprosthetic valves do not require lifelong blood thinners, but they have a finite lifespan and are prone to structural wear over time. In this case the valve degenerated approximately three to four years after implantation. Its leaflets stiffened and could no longer open and close normally, a finding confirmed on 2D echocardiography. Further evaluation revealed a second, separate problem: significant blockages had developed in the coronary arteries supplying the heart muscle, confirmed on coronary angiography.
Emotional and psychological impact
Facing a second open-heart operation within a few years of the first is a daunting prospect for any patient. As the bioprosthesis failed, the patient developed breathlessness on exertion and episodes of chest pain — symptoms that limit everyday activity and can be distressing to live with. The return of a heart problem that had previously been corrected carries a real psychological burden, compounded by understandable anxiety about undergoing a more complex redo procedure combined with bypass surgery.
What was assessed during the consultation
Why this approach was chosen
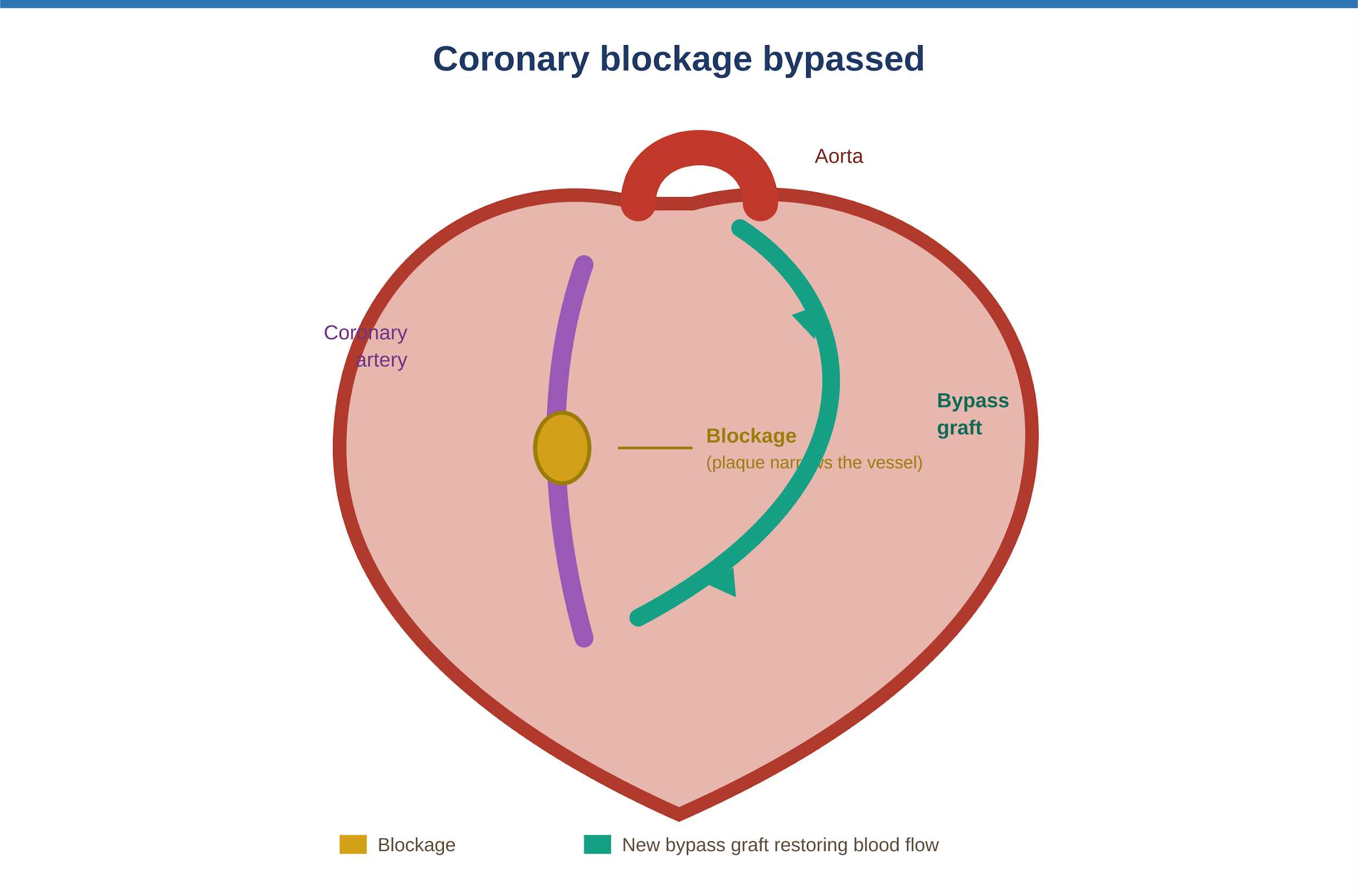
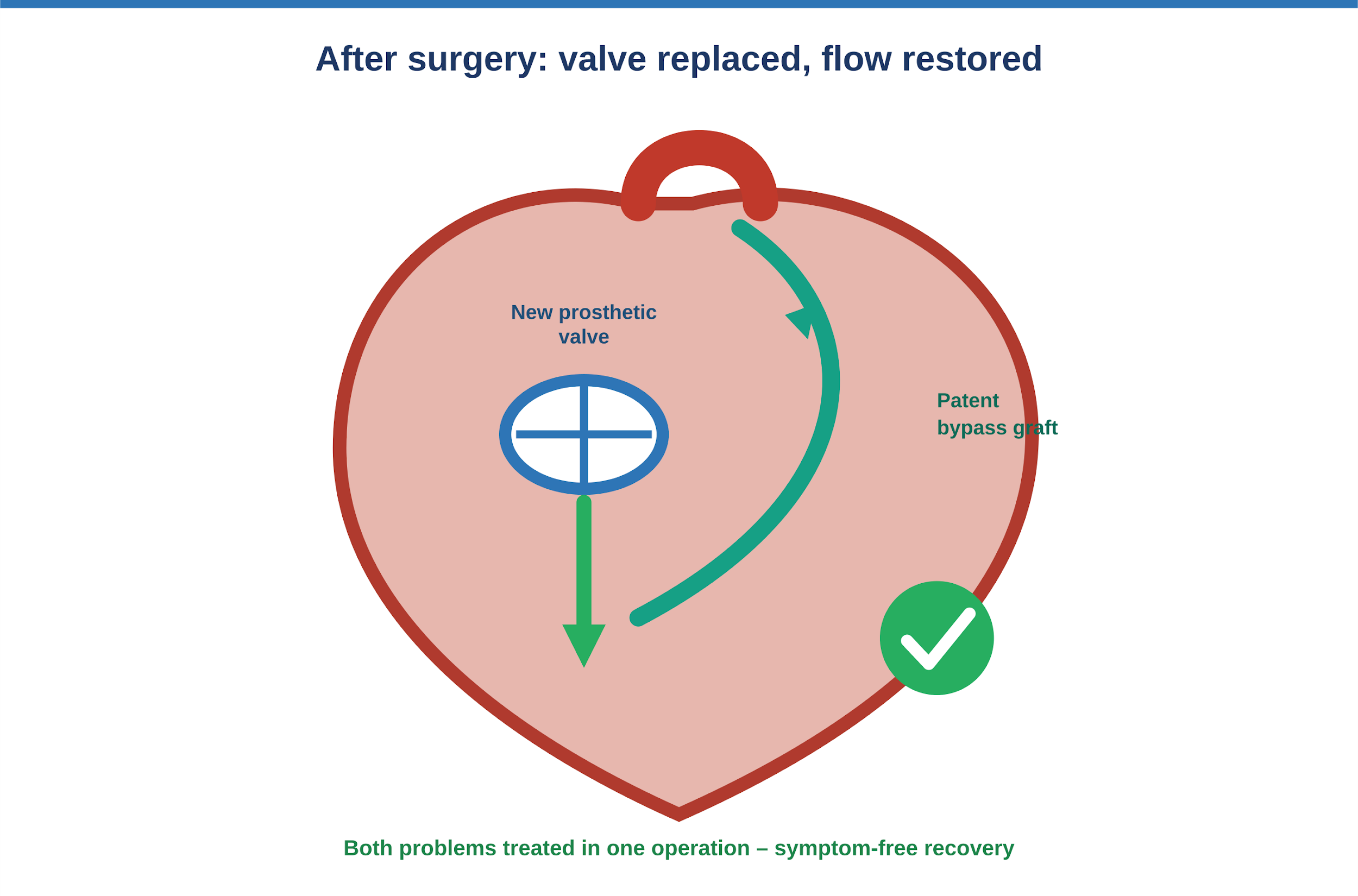
Dr. Vishal Khullar counsels patients that there is no single “ideal” prosthetic valve. Tissue valves and mechanical valves each carry their own advantages and trade-offs. Here, two problems had to be resolved in a single operation:
For a case of this kind, the key baseline documentation is the 2D echocardiogram, showing the degenerated mitral bioprosthesis, and the coronary angiogram, showing the vessel blockages. Together these confirm the diagnosis and define the surgical plan.
![P1]](https://drvishalkhullar.com/wp-content/uploads/p1-5.png)
Step-by-step overview
Procedure facts
|
Procedure |
Redo mitral valve replacement + coronary artery bypass grafting (CABG) |
|
Duration |
Approximately 5 to 6 hours |
|
Anaesthesia |
General anaesthesia |
|
Valve used |
Mechanical bileaflet mitral valve, 29 mm |
|
Approach / incision |
Redo sternotomy (re-opening of previous midline chest incision) |
|
Intraoperative complications |
None: surgery completed without complications |
|
Hospital stay |
8 to 10 days |
A related video from Dr. Vishal Khullar accompanies this case, walking through the entire process from consultation to recovery.
Today I feel stronger and able to return to my daily routine at home. I’m deeply grateful to Dr. Vishal Khullar and his team for giving me a renewed sense of health and a second chance. I wouldn’t hesitate to recommend him to anyone facing complex heart surgery.”
Instructions typically given after this procedure
The points below reflect standard post-cardiac-surgery guidance. The exact instructions given to this patient should be confirmed against her discharge summary.
Procedure Facts
|
PROCEDURE |
Beating heart (off pump) coronary artery bypass grafting |
|
ANAESTHESIA |
General anaesthesia |
|
GRAFTS USED |
Internal mammary (internal thoracic) arterial grafts |
|
APPROACH |
Off pump. Surgery performed on the beating heart without a heart lung machine |
|
INTRAOPERATIVE COMPLICATIONS |
None reported |
|
HOSPITAL STAY |
Discharged on post operative day 5 |
The post operative course was smooth and uneventful. The patient was mobilised early, walking in the ICU within two days of surgery, and was discharged on the fifth post operative day. By around the fifteenth day his sutures had been removed and he was walking comfortably and managing daily activities independently. For patients at this stage, the practical guidance on recovering from heart surgery covers what to expect and which warning signs to watch for. The surgical goal of restoring reliable blood supply to the heart with durable arterial grafts was fully achieved.
|
Timeframe |
What the patient can expect |
|
Day 1–3 |
Initial recovery, often beginning in intensive care; close monitoring and gradual mobilisation. |
|
Week 1–2 |
Discharge home for most patients; wound and suture checks; light activity around the house. |
|
Week 4–6 |
Continued healing of the sternum; everyday activities gradually resumed within sternal precautions. |
|
Month 3 |
Most patients feel substantially better; cardiac rehabilitation progressing; lighter exercise reintroduced. |
|
Month 6 |
Recovery generally well established; valve and graft function reviewed at follow-up. |