Trusted By
9,000+ Patients Globally
A 52-year-old patient with severe shortness of breath, infective endocarditis, and a 50 mm ascending aortic aneurysm — treated by Dr. Vishal Khullar at Nanavati Max Super Speciality Hospital, Mumbai.
The following clinical profile was prepared in line with Indian medical confidentiality guidelines. The patient consented to publication of his case for educational and clinical record purposes. His identity has been withheld.
|
Age |
52 years |
|
Gender |
Male |
|
Occupation |
Working professional |
|
City |
Maharashtra (suburban region) |
|
Presenting Complaint |
Severe shortness of breath, reduced exertional tolerance |
|
Diagnosis |
Bicuspid aortic valve with ascending aortic aneurysm and infective endocarditis with aortic regurgitation |
|
Duration of Issue |
Progressive symptoms over several months prior to admission |
|
Previous Treatments |
Initial evaluation at a local hospital, including CT scan and echocardiography. No definitive surgical intervention prior to referral. |
|
Date of Procedure |
Recent surgical intervention |
|
Outcome |
Excellent — uneventful recovery, no post-operative complications |
Patient identity withheld per confidentiality guidelines. Case published with documented consent.
Clinical Condition
The patient was diagnosed with three overlapping cardiac conditions, each of which carried independent surgical urgency. The combination made the case unusually complex.
The first finding was a bicuspid aortic valve, a congenital condition in which the valve has only two leaflets instead of the usual three. This abnormal structure had been present since birth, and over decades it had begun to fail mechanically. The second finding was an ascending aortic aneurysm measuring 50 millimetres, well above the 45 to 50 mm surgical threshold recommended by current cardiothoracic guidelines. Earlier imaging at the patient’s local hospital had estimated the aneurysm at 28 mm, indicating rapid progression. The third finding, and the most acute, was infective endocarditis affecting the aortic valve. Bacterial vegetations had destroyed parts of the leaflet tissue and the valve had begun to leak severely. Blood was flowing backward into the heart with every contraction.
Emotional and Psychological Impact
By the time the patient reached Mumbai, his breathlessness had become severe enough to limit ordinary movement around the house. The family described a period of considerable anxiety. They had visited a local hospital first, where a CT scan and echocardiography revealed the aortic leak. A relative referred them to Nanavati Hospital and to Dr. Vishal Khullar.
The family arrived without a clear understanding of what surgery would involve or what the recovery would look like. The diagnosis itself was difficult to accept, given that the patient had appeared otherwise healthy until the breathlessness began. The clinical team focused early consultations on patient and family education, recognising that informed consent for a procedure of this magnitude required time and clarity.
Pre-Surgical Assessment by Dr. Vishal Khullar
The patient underwent a complete cardiac and aortic workup before any surgical decision was made. The assessment was structured to clarify the severity of each condition and to establish whether a single combined operation was both feasible and safer than staged procedures.
Why a Combined Procedure Was Chosen
Several treatment paths were considered. Dr. Khullar’s team weighed the risks of staged surgery against a single combined operation. The combined approach was selected for the following clinical reasons.
The plan was finalised after a multidisciplinary discussion involving cardiac anaesthesia, perfusion, and intensive care teams. The patient and his family were counselled in detail about the planned circulatory arrest, the use of a vascular graft, and the prosthetic valve options.
Imaging confirmed the diagnostic triad. The illustration below summarises the anatomical findings observed on transthoracic echocardiography and CT aortogram.
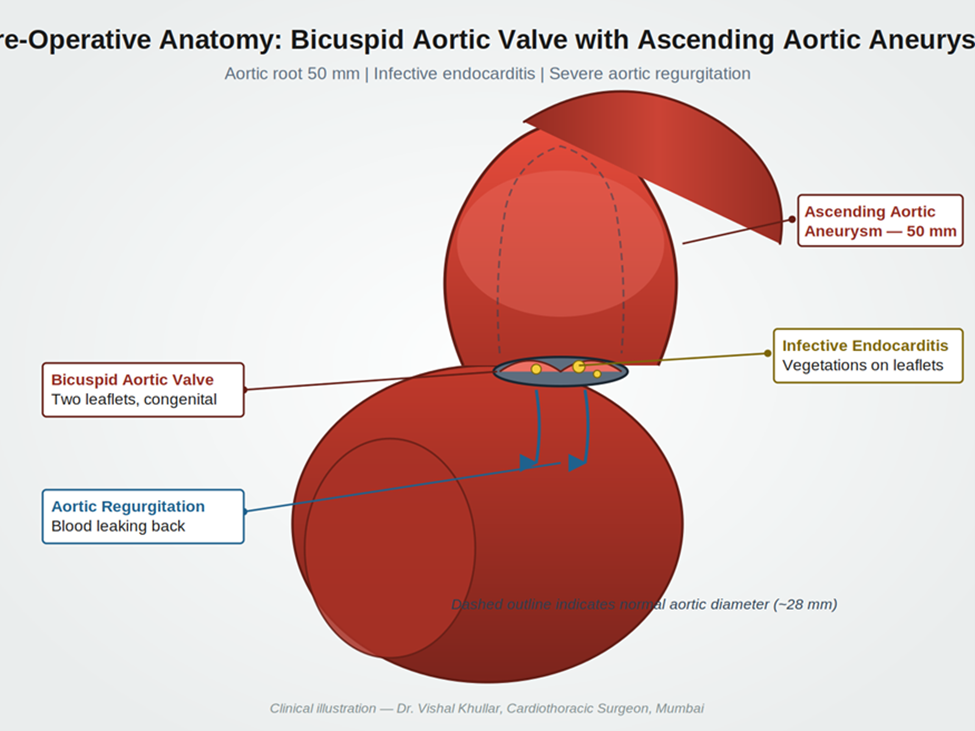
Figure 1. Pre-operative anatomy showing bicuspid aortic valve with infective vegetations, ascending aortic aneurysm at 50 mm, and severe aortic regurgitation.
Step-by-Step Surgical Overview
Procedure Facts
|
Duration |
Approximately 6 to 7 hours |
|
Anaesthesia |
General anaesthesia with invasive haemodynamic monitoring |
|
Implants Used |
Mechanical bileaflet aortic valve prosthesis and Dacron ascending aortic graft |
|
Approach |
Median sternotomy with cardiopulmonary bypass |
|
Circulatory Arrest |
24 minutes with selective antegrade cerebral perfusion |
|
Intraoperative Complications |
None |
|
Hospital Stay |
Three days in ICU followed by ward recovery |
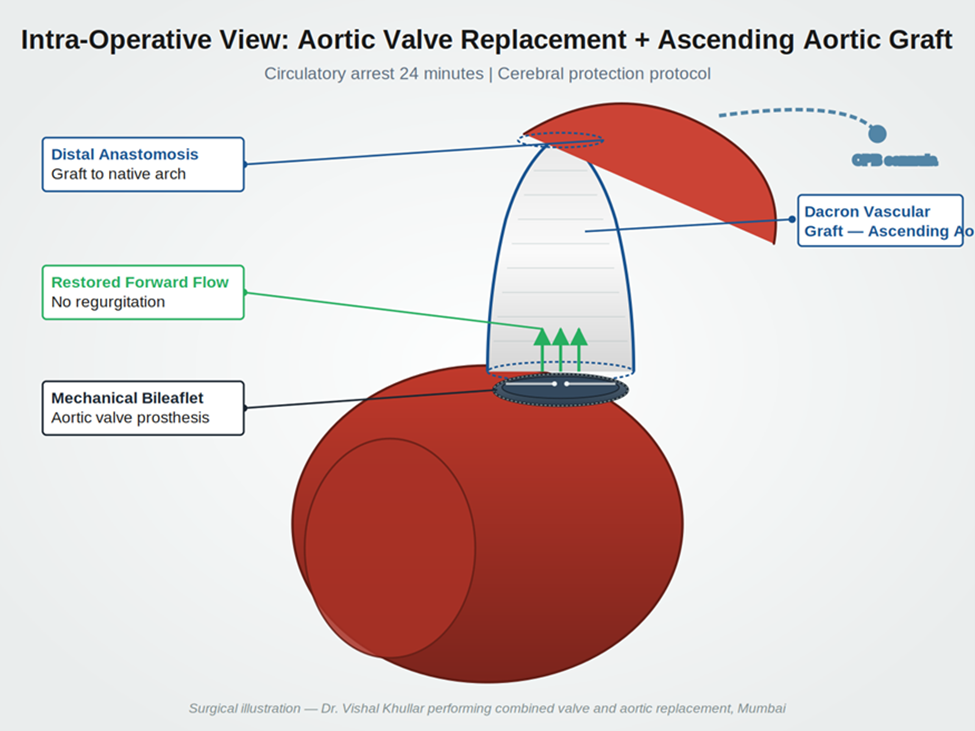
Figure 2. Intraoperative reconstruction. The ascending aorta has been replaced with a Dacron graft and the bicuspid aortic valve has been replaced with a mechanical bileaflet prosthesis.
The combined procedure achieved its three primary objectives. The infected aortic valve was completely excised and replaced with a competent prosthesis. The dilated ascending aorta was replaced with a vascular graft, removing the risk of dissection. Forward blood flow from the left ventricle to the systemic circulation was restored. Aortic regurgitation was eliminated.
Post-operative recovery was uneventful. The patient was extubated on post-operative day one. He was shifted out of the ICU on post-operative day three. There were no surgical, neurological, or infective complications.
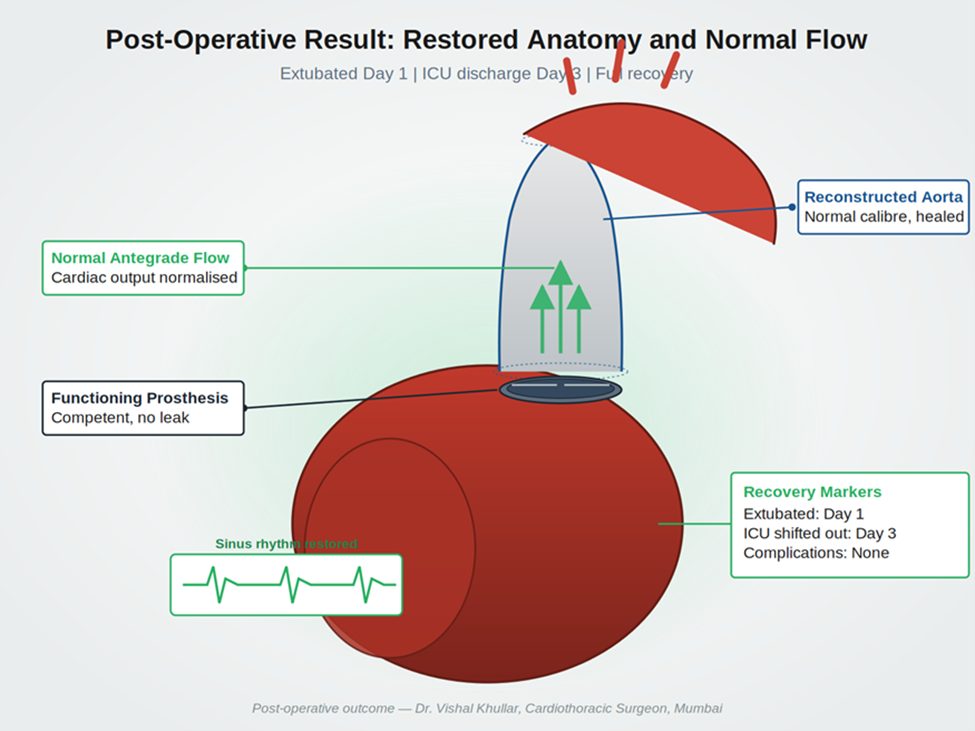
Figure 3. Post-operative result. Reconstructed aortic anatomy with normal calibre, functioning prosthetic valve, and restored sinus rhythm.
Outcomes at a Glance
|
Outcome Metric |
Result |
|
Symmetry and Cardiac Function |
✓ Excellent. Sinus rhythm restored on weaning from bypass. |
|
Surgical Outcome |
✓ Complete excision of infected tissue and aneurysmal segment. |
|
Patient Recovery |
✓ Smooth and uncomplicated. Family confirmed full symptom resolution. |
|
Complications |
✓ None during ICU stay or ward recovery. |
|
Recovery Trajectory |
✓ On track. Discharged within the expected timeframe. |
The following feedback was recorded during the patient’s clinical follow-up. It has been transcribed from the family’s original words. Minor language corrections have been made for readability while preserving the substance of what was said. A video recording of the patient’s family and Dr. Vishal Khullar narrating the case is included below.
|
My son had been suffering for some time. We took him to a local hospital first. They did a CT scan and a sonography. After the sonography, they told us there was a leak in his heart valve. We were worried. A relative gave us a letter for Nanavati Hospital and told us to consult Dr. Vishal Khullar. We met the doctor. He explained that surgery was needed. He said there was no other option. The aneurysm had grown to 50 millimetres. After the operation, my son recovered completely. We are grateful to the doctor and his team. — Father of the patient — recorded during follow-up review |
Watch the patient’s family and Dr. Vishal Khullar describe the case in their own words:
▶ WATCH THE FULL CASE NARRATION
Bicuspid Aortic Valve with Ascending Aortic Aneurysm and Infective Endocarditis — Patient Family and Dr. Vishal Khullar
Surgeon’s clinical note on the case:
The patient was a 52-year-old male who presented with severe shortness of breath. He was diagnosed with a bicuspid aortic valve, ascending aortic aneurysm, and infective endocarditis of the aortic valve. The infection had caused the valve to leak. Blood was flowing back into the heart with each contraction. To replace the diseased aortic segment, we had to stop body circulation for 24 minutes. This is a high-risk operation because the brain and several internal organs are vulnerable to ischaemia, and their function must be actively protected. After surgery the patient did well. He was extubated on post-operative day one. There were no complications. He was shifted out of the ICU on post-operative day three.
— Dr. Vishal Khullar, Cardiothoracic Surgeon, Nanavati Max Super Speciality Hospital, Mumbai
Discharge Instructions Given to the Patient
Recovery Timeline
|
Timeframe |
What the Patient Could Expect |
|
Day 1 to 3 |
ICU recovery. Extubation on day one. Haemodynamic stabilisation. Transition to ward by day three. |
|
Week 1 to 2 |
Ward recovery. Anticoagulation started and titrated. Antibiotic regimen continued. Sutures and drains removed in stages. |
|
Week 4 to 6 |
Light activity at home. Cardiac rehabilitation initiated. First post-discharge follow-up at week two, then week six with echocardiography. |
|
Month 3 |
Return to most non-strenuous routine activities. Sternal healing complete. INR stable on home monitoring. |
|
Month 6 |
Six-month review with echocardiography. Prosthesis function confirmed. Patient discharged from active surgical follow-up to long-term cardiology care. |
Q1. What is a bicuspid aortic valve and why does it need surgery?
A bicuspid aortic valve is a congenital condition in which the valve forms with only two leaflets instead of the usual three. Many people live with it for decades without symptoms. Over time the valve can become stiff, leak, or develop infections, and it is also linked to enlargement of the ascending aorta. When complications develop, surgical repair or replacement is needed. Dr. Vishal Khullar performs bicuspid aortic valve surgery at Nanavati Max Super Speciality Hospital in Mumbai.
Q2. Why was both the valve and the aorta replaced in the same operation?
When a bicuspid valve is associated with an ascending aortic aneurysm above 45 to 50 millimetres, current cardiothoracic guidelines recommend repairing both at the same time. This avoids a second high-risk surgery within months and addresses the dissection risk before it can rupture. In this case the aneurysm measured 50 millimetres and the valve was acutely infected, which made a single combined procedure the safer route.
Q3. What is circulatory arrest and how is it carried out safely?
Circulatory arrest is a controlled period during open aortic surgery in which body circulation is briefly stopped. It allows the surgeon to operate on a bloodless aortic field. Patient safety depends on deep cooling and on selective perfusion of the brain. In this case, body circulation was stopped for 24 minutes while cerebral perfusion was preserved. The technique is high-risk and is performed at centres with experienced aortic teams.
Q4. How long does recovery take after combined valve and aortic graft surgery in Mumbai?
Most patients spend two to three days in the ICU and another seven to ten days in the ward. Sternal healing takes around six weeks. Light routine activity returns within two to three months, and full recovery with cardiac rehabilitation is usually complete by the six-month mark. Patients on a mechanical valve continue lifelong anticoagulation under medical supervision. Specific timelines can vary, and the cardiac team at Nanavati Max Super Speciality Hospital in Mumbai sets follow-up schedules to suit each case.
Q5. Why choose Dr. Vishal Khullar for complex aortic and valve surgery?
Dr. Vishal Khullar is the Director of Cardiovascular and Thoracic Surgery, Heart and Lung Transplantation, and Mechanical Circulatory Support at Nanavati Max Super Speciality Hospital in Mumbai. He trained and held senior positions at Mayo Clinic in Rochester and Cleveland Clinic in Ohio. His surgical experience covers more than 7,000 cardiac operations, including complex aortic procedures, infective endocarditis, redo cardiac surgery, and heart and lung transplantation. He works with a multidisciplinary aortic team, which is the appropriate setting for cases of this complexity.